












Deprecated: htmlspecialchars(): Passing null to parameter #1 ($string) of type string is deprecated in /bitnami/joomla/modules/mod_search/mod_search.php on line 44

Admin Login
Translate Languages
Warning: Undefined variable $panel in /bitnami/joomla/administrator/components/com_widgetkit/plugins/widgets/grid/views/widget.php on line 125
Warning: Undefined variable $panel in /bitnami/joomla/administrator/components/com_widgetkit/plugins/widgets/grid/views/widget.php on line 126

ACT Trial
ACT: QuICR & OPTIMISE is a Pragmatic Phase III randomized open-label registry-based trial with blinded end-point assessment. Enrolled acute ischemic stroke patients will be eligible to receive intravenous thrombolysis (Alteplase or Tenecteplase) as per current guidelines. Over the three year study period, 1,600 patients will be treated with tPA or TNK, with followup at 90 days. The primary outcome measure will be a modified Rankin Scale (mRS) 0 or 1 at 90-120 days.
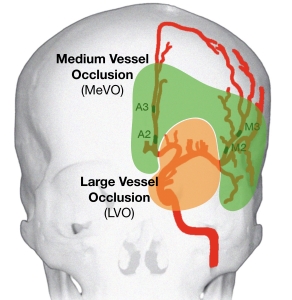
MEVO Frontiers - Medium Vessel Occlusion
While current guidelines do not recommend endovascular treatment for MeVOs, techniques are improving rapidly, making these occlusions more safely accessible. As such, clinical practice is evolving, and MeVOpatients are increasingly being treated. This practice is heterogeneous though, and experiences are not reported on a large scale. We think that treatment of these patients could be the next frontier in improving outcomes of acute stroke.
ESCAPE NEXT
The ESCAPE NEXT Trial is a multicentre, randomized, double-blinded, placebo-controlled, parallel group, single-dose design to determine the efficacy and safety of intravenous Narinitide in subjects with acute ischemic stroke not recieving or ineligable for alteplase undergoing endovascular thrombectomy.

DESTINY Survey on Treating Unruptured aneurysms
Survery of neurinterventionalists and Neurosurgeons regarding factors affecting the Treatment of Unruptured Intracranial Aneurysms

ALICE in Wonderland Survey of Neurointerventionalists
Survey conducted during the ALICE Course 2019 in Essen Germany in collaboration with Rene Chapot. Results are published in multiple journals.

EVOLVE - ASA vs Placebo for Unruptured Aneurysm Coiling

ESCAPE NA-1
To determine the efficacy of the neuro protctant NA-1 in reducing global disability in subjects with AIS with a small established infarct core and good collateral circulation selected for EVT.
The study has concluded with results published in the Lancet.

UNMASK EVT
An international multidisciplinary survey to examine decisions in EVT care across the world. What factors govern the selection for EVT in the real-world.

TEMPO 2 Study
To demonstrate the efficacy of using TNK-tPA to treat minor ischemic stroke in proven arterial occlusion.
A Phase 3, prospective, randomized controlled, open-‐label with blinded outcome assessment (PROBE) controlled trial.

DATAS II
Establish the safety of early anticoagulation with the novel oral anticoagulant dabigatran in acute cerebrovascular syndrome patients.
Identify the rate of both symptomatic and asymptomatic hemorrhagic transformation (HT) associated with these treatments.
Identify predictors of HT associated with acute dabigatran treatment.
Hypothesis: The Investigators hypothesize that symptomatic HT rates in dabigatran and ASA treated patients will not be significantly different.

